Empowering Shared Decision-Making in Medical Education: The B.R.A.I.N. Framework for doctor-patient consultations

Shared decision making (SDM) is a cornerstone of patient-centred care, a key focus in NHS policy, GMC guidance, and NICE recommendations. Yet, despite its importance, many clinicians and medical students find shared decision making challenging to implement in real-world consultations. At Norwich Medical School, we’ve responded to this challenge by introducing the B.R.A.I.N. framework—a practical, memorable tool to support shared decision making conversations and help future doctors deliver truly universal personalised care.
Why Focus on Shared Decision-Making?
The principle of “No decision about me, without me” is now embedded in UK healthcare, reflecting a shift towards partnership between patients and clinicians. The NHS Long Term Plan and NICE guidelines both emphasise the need for patients to be informed and actively involved in decisions about their care. With the GMC stating that shared decision making should take place with ‘all patients, in all settings, for all decisions—from routine to complex, except where the patient lacks capacity or in emergencies’. However, barriers remain:
- Lack of clear tools and resources for structuring SDM conversations
- Uncertainty about how to discuss risks, benefits, and alternatives
- Institutional pressures, time constraints, and complex terminology
- Students reporting lower confidence and performance in SDM skills compared to other consultation skills
Our own student feedback echoed these challenges, with many requesting more guidance and structure for SDM, especially when moving from information-giving to a more collaborative approach.
Introducing the B.R.A.I.N. Framework
To address these needs, we introduced the B.R.A.I.N mnemonic, adapted from the Choosing Wisely UK campaign and childbirth education resources, and tailored specifically for undergraduate medical education. Unlike a traditional decision aid, this tool is designed for clinicians to use directly during doctor-patient consultations. B.R.A.I.N stands for; Benefits, Risks, Alternatives, Intuition, (do) Nothing.
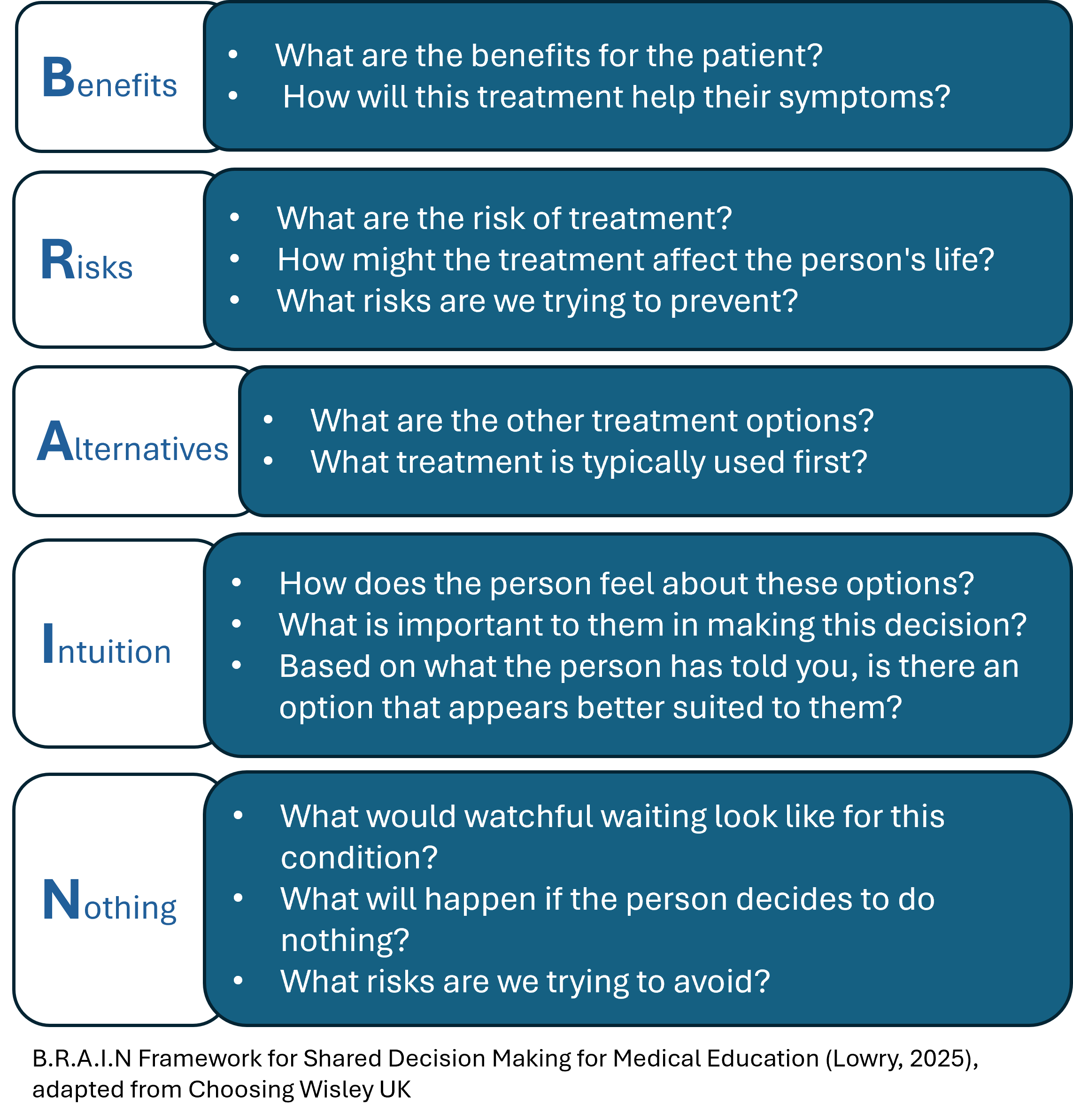
Figure 1. B.R.A.I.N a framework for doctors to help facilitate shared decision making conversations.
This framework helps medical students and clinicians move beyond simply listing treatment options. Instead, it encourages them to focus on what truly matters to each individual patient. The B.R.A.I.N framework is designed to support clinicians in explaining treatment and care plans in a way that fosters genuine collaboration and partnership. By using this approach, both clinician and patient work together to build a shared understanding and make decisions about care as a team.
Integrating B.R.A.I.N. with the Calgary-Cambridge Guide we embedded B.R.A.I.N. within the established Calgary-Cambridge consultation model, ensuring that SDM is not a standalone skill but integrated throughout the consultation. Students are encouraged to:
- Set the agenda and invite the patient to participate in decision making
- Gather the patient’s perspective using ICE (Ideas, Concerns, Expectations)
- Clearly explain the details of the condition and all available options
- Use B.R.A.I.N. to structure the discussion, check understanding, and explore patient preferences
- Build rapport by actively listening, picking up on cues, and showing empathy

Figure 2. B.R.A.I.N integrated with the Calgary Cambridge Guide, demonstrating the key skills needed for successful shared decision making conversation.
This approach helps medical students develop a logical, patient-centred sequence for consultations, while also supporting the development of communication skills that are essential for safe and effective practice.
Early Impact and Evaluation
Since introducing B.R.A.I.N., we have trained over 600 third-year undergraduate medical students, with positive feedback from students, simulated patients, and tutors alike. Students report greater confidence in structuring SDM conversations, and our student evaluation data suggests significantly improved satisfaction with their teaching and practice compared to previous models used. We are currently evaluating the impact of B.R.A.I.N using a mixed-methods, pre/ post-intervention design including student evaluations, simulated patient and tutor surveys with collaborators Dr Susan Miles & Dr Sadie Lawes-Wickwar – watch this space for publication!
Looking Ahead
The B.R.A.I.N. framework is already making a difference at Norwich Medical School, supporting a new generation of clinicians to have more meaningful, collaborative conversations with patients. By empowering medical students to explore not just the clinical facts, but also the patient’s values, preferences, and intuition, we are helping to deliver truly personalised care.
We believe that sharing practical tools like B.R.A.I.N can help bridge the gap between policy and practice, and we would welcome collaboration with colleagues across the UK and beyond to integrate this approach for better patient outcomes.
Interested in learning more or collaborating?
Contact Dr Ellen Lowry at e.lowry@uea.ac.uk.
Conference presentation slides [downloads PowerPoint file]
Ellen Lowry is a Chartered Psychologist and Behavioural Scientist working at the intersection of cognitive neuroscience, medical education, and clinical communication. She applies rigorous experimental principles to design and evaluate innovative educational interventions that enhance patient experience and support clinician development. Her translational research bridges the gap between theory and practice, focusing on behavioural change, health promotion, Shared Decision Making, and person-centred communication to strengthen patient interactions and improve health outcomes.
Share this blog post:
Featured blog posts:

Flourishing Spaces: Small acts of resistance – A UKCCC Guest Blog by Professor Louise Younie

Empowering Shared Decision-Making in Medical Education: The B.R.A.I.N. Framework for doctor-patient consultations

Why Should We Teach Empathic Communication Skills to Medical Students?
Contact Us